

Start making more connections & convert more sales
1
Setup in minutes
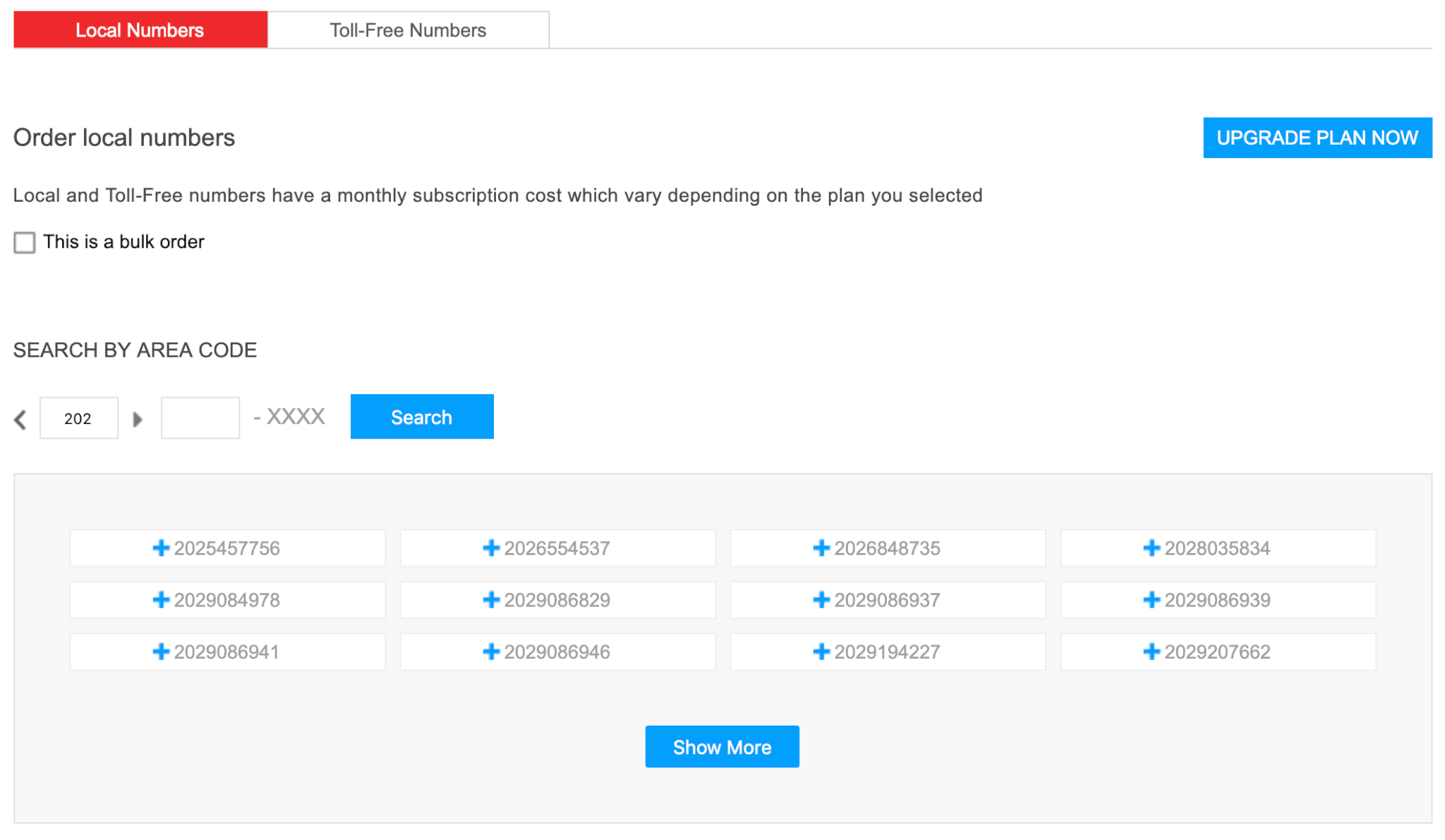
No hardware. No headaches. Just a beautiful cloud-based solution you can use to connect with your customers immediately.
2
Connect your tools
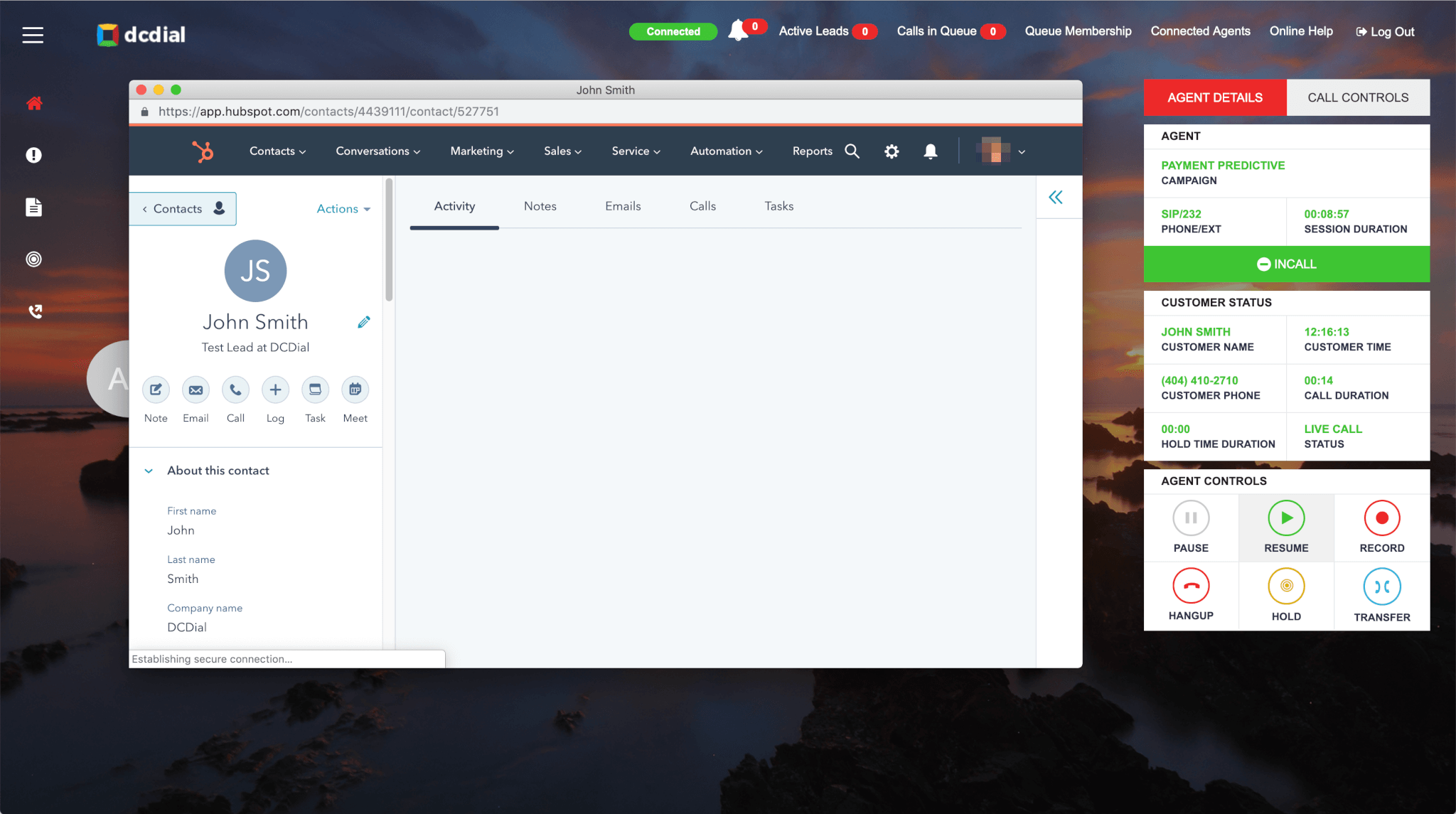
Calls go better when all the right info is tied together. Integrate DCDIAL with CRM systems, sales & marketing solutions, and other essential apps.
3
Boost engagement
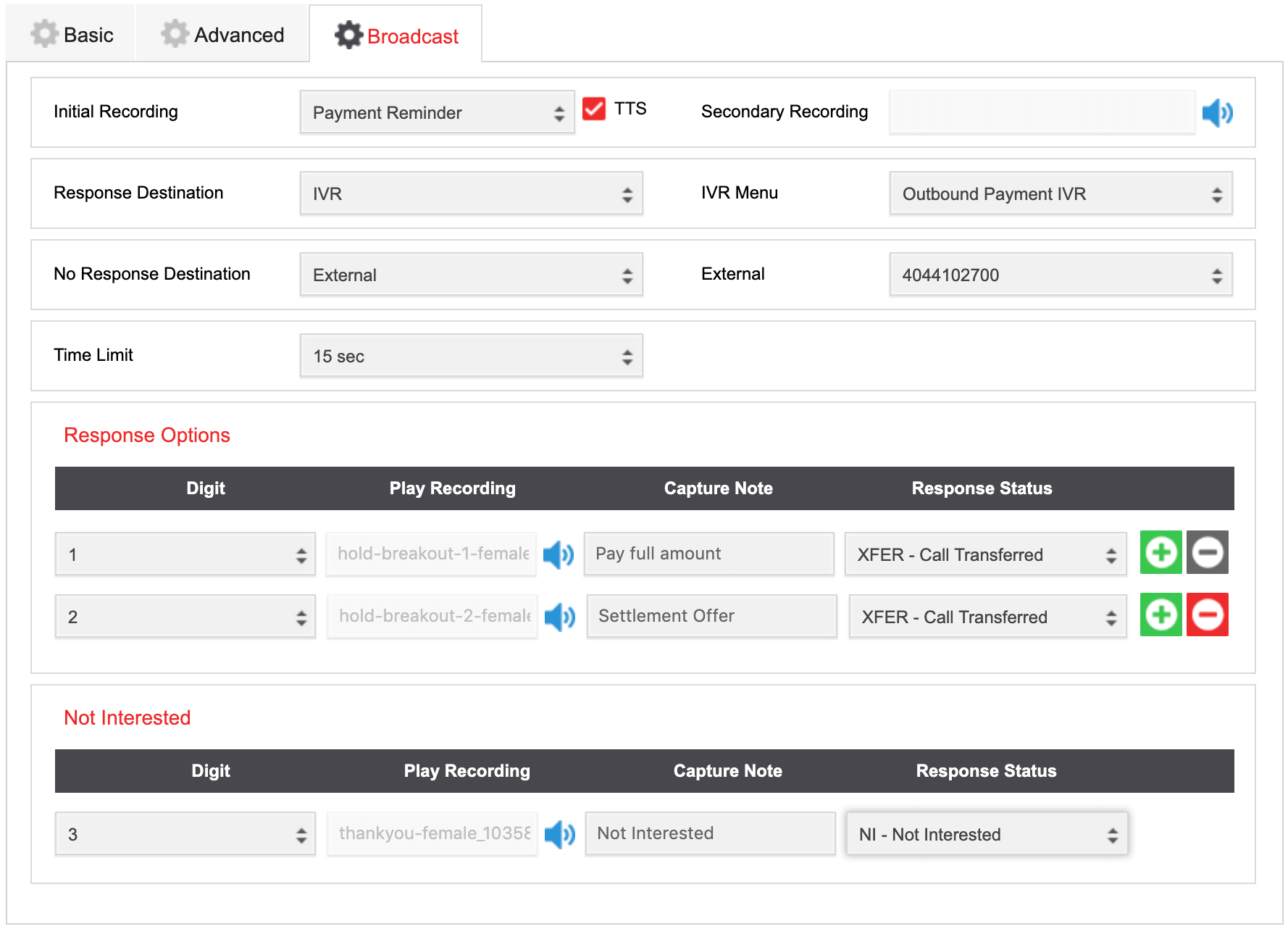
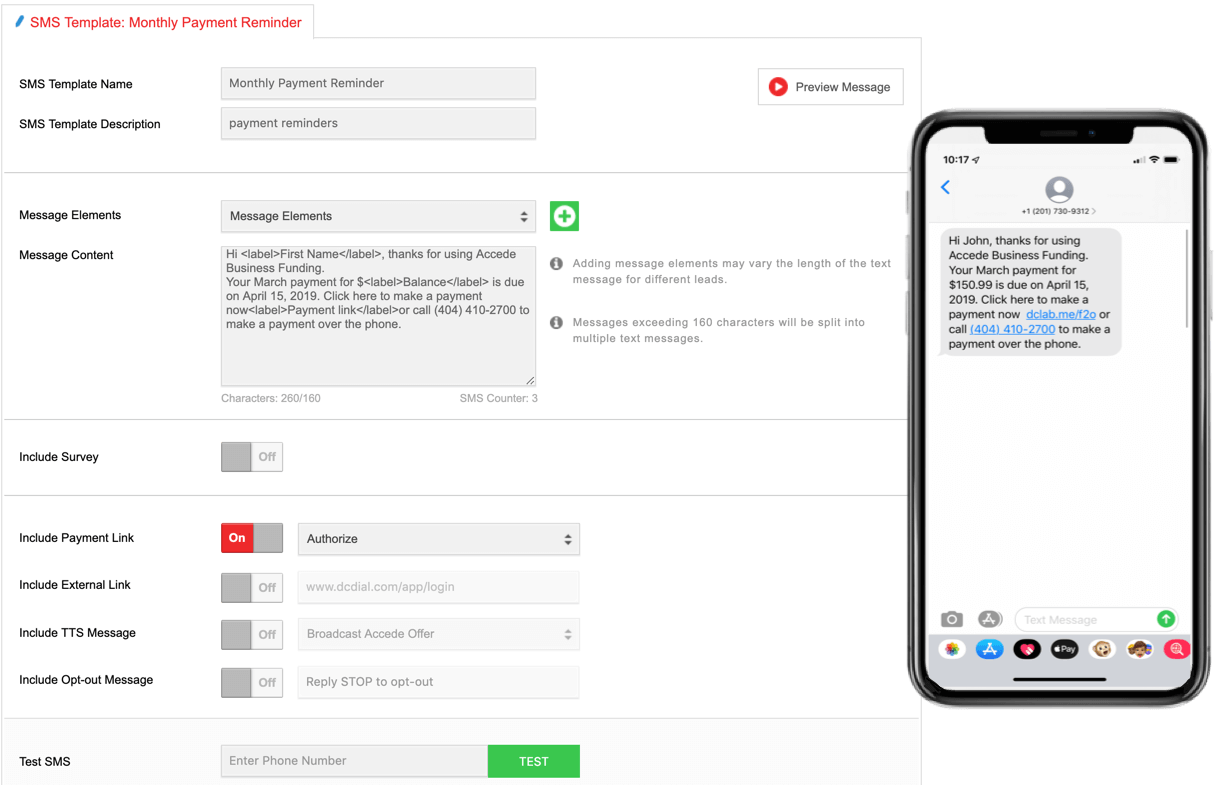
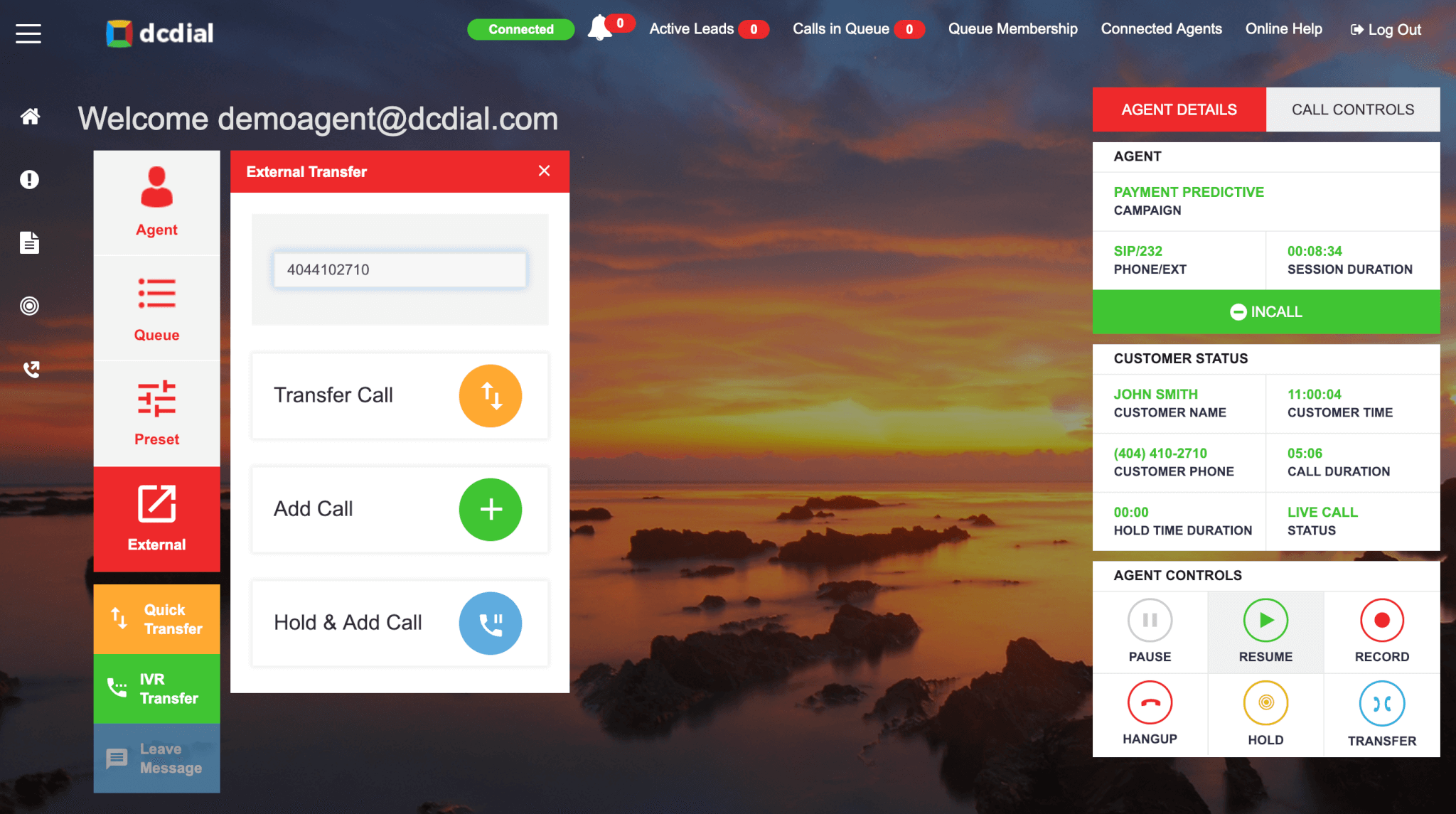
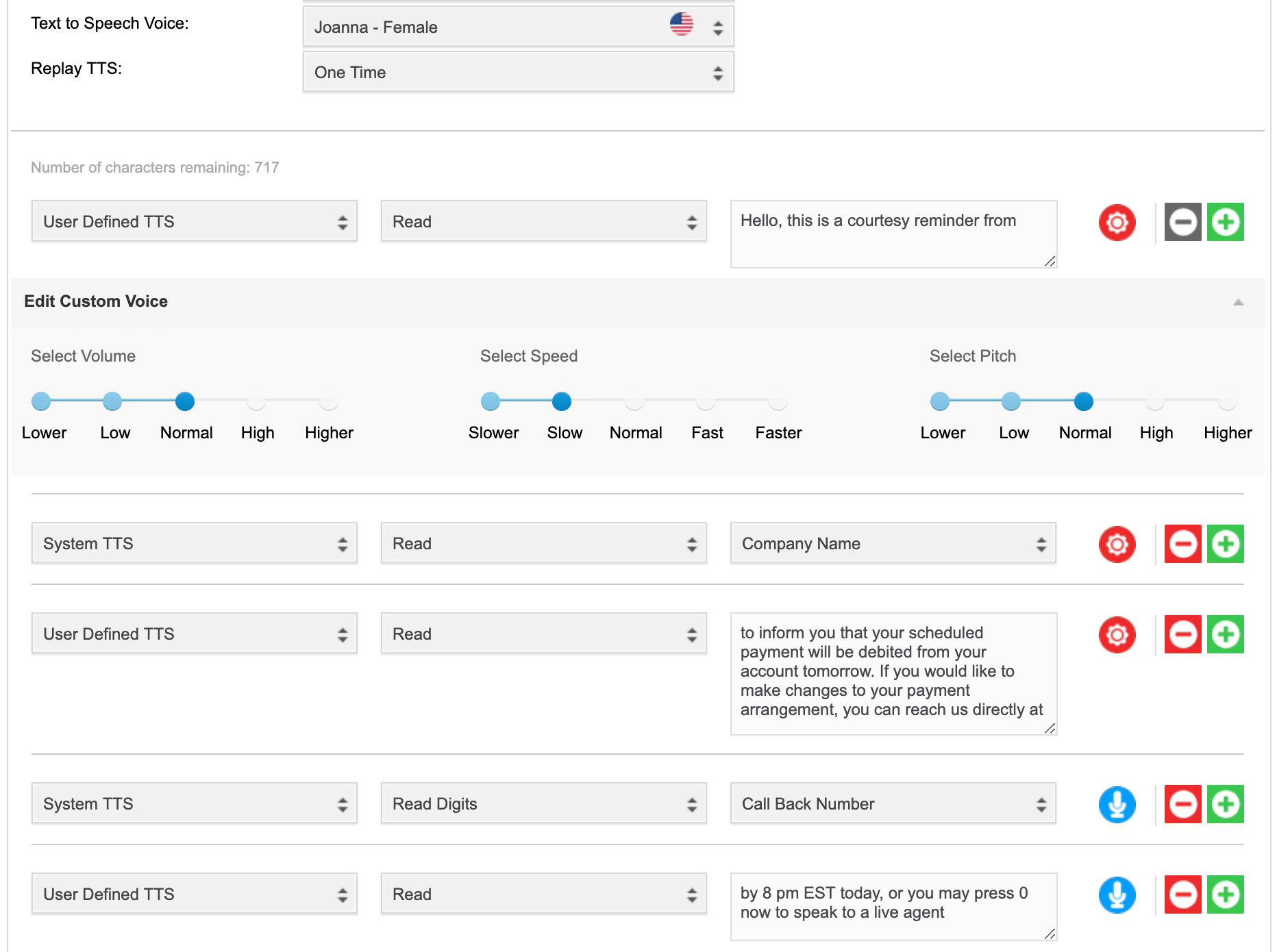
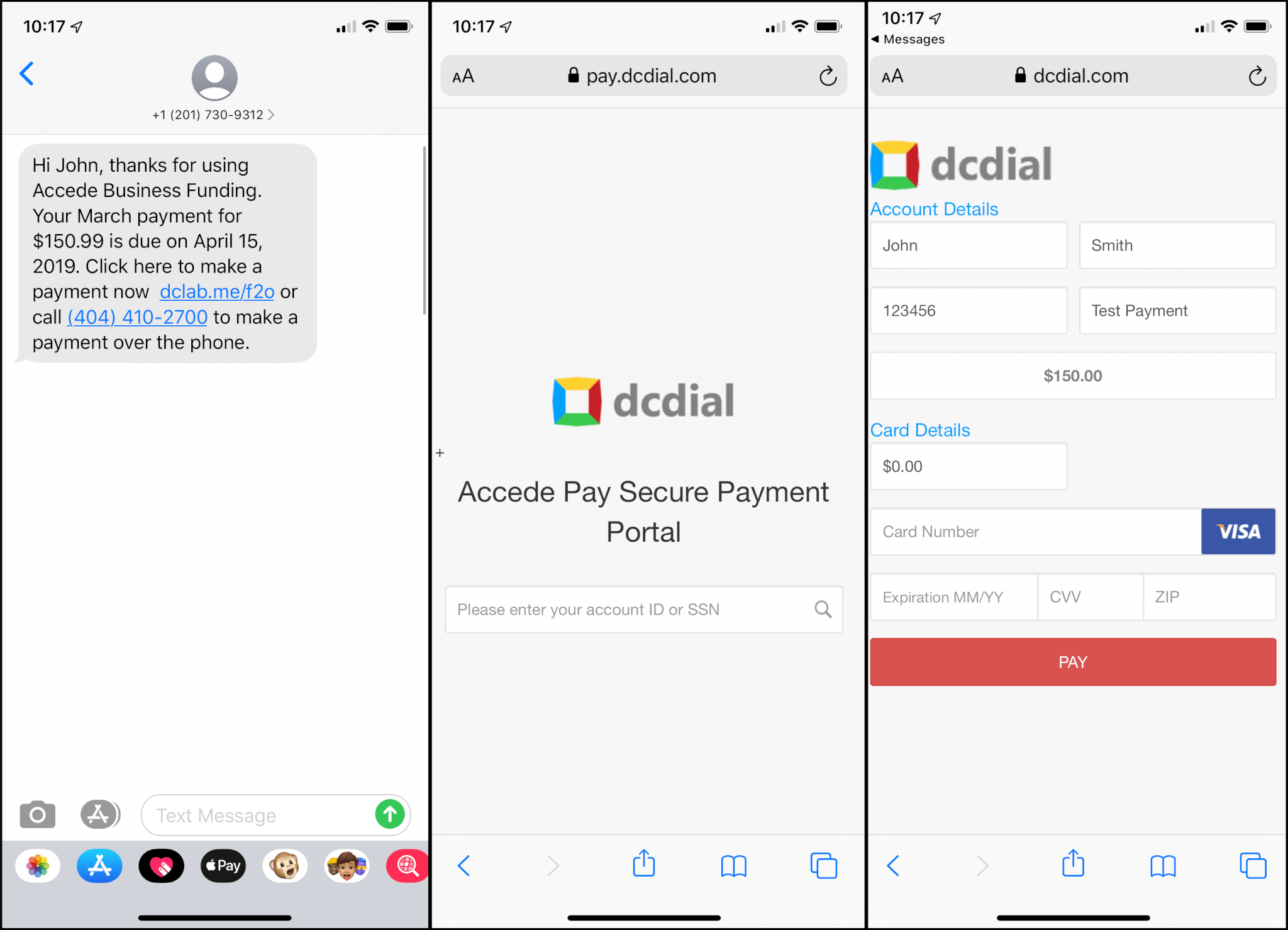
Connect your agents with live customers faster, smarter, and with higher closing rates. Send personalized voice and text messages to thousands of customers in minutes.
4
Increase revenue
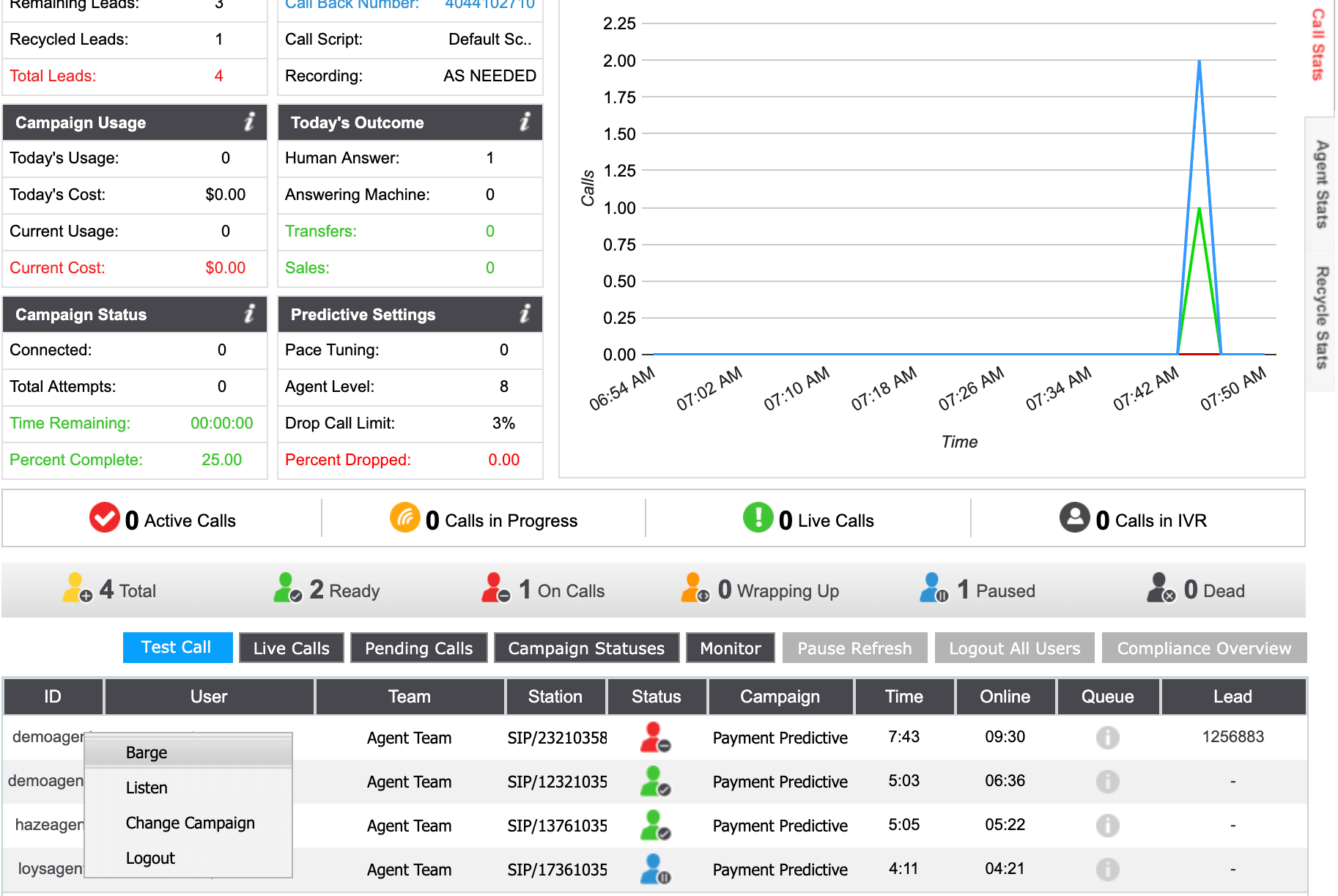
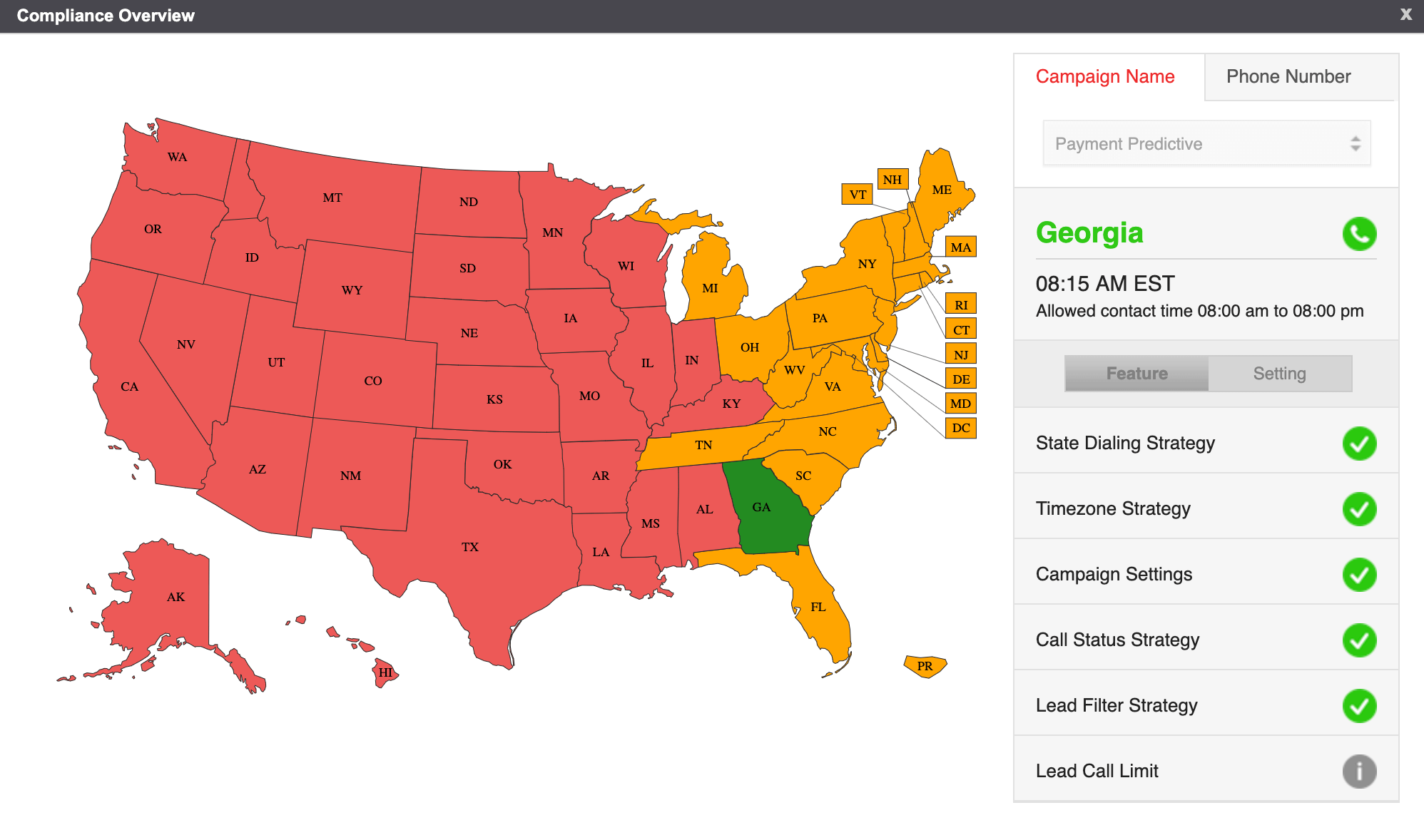
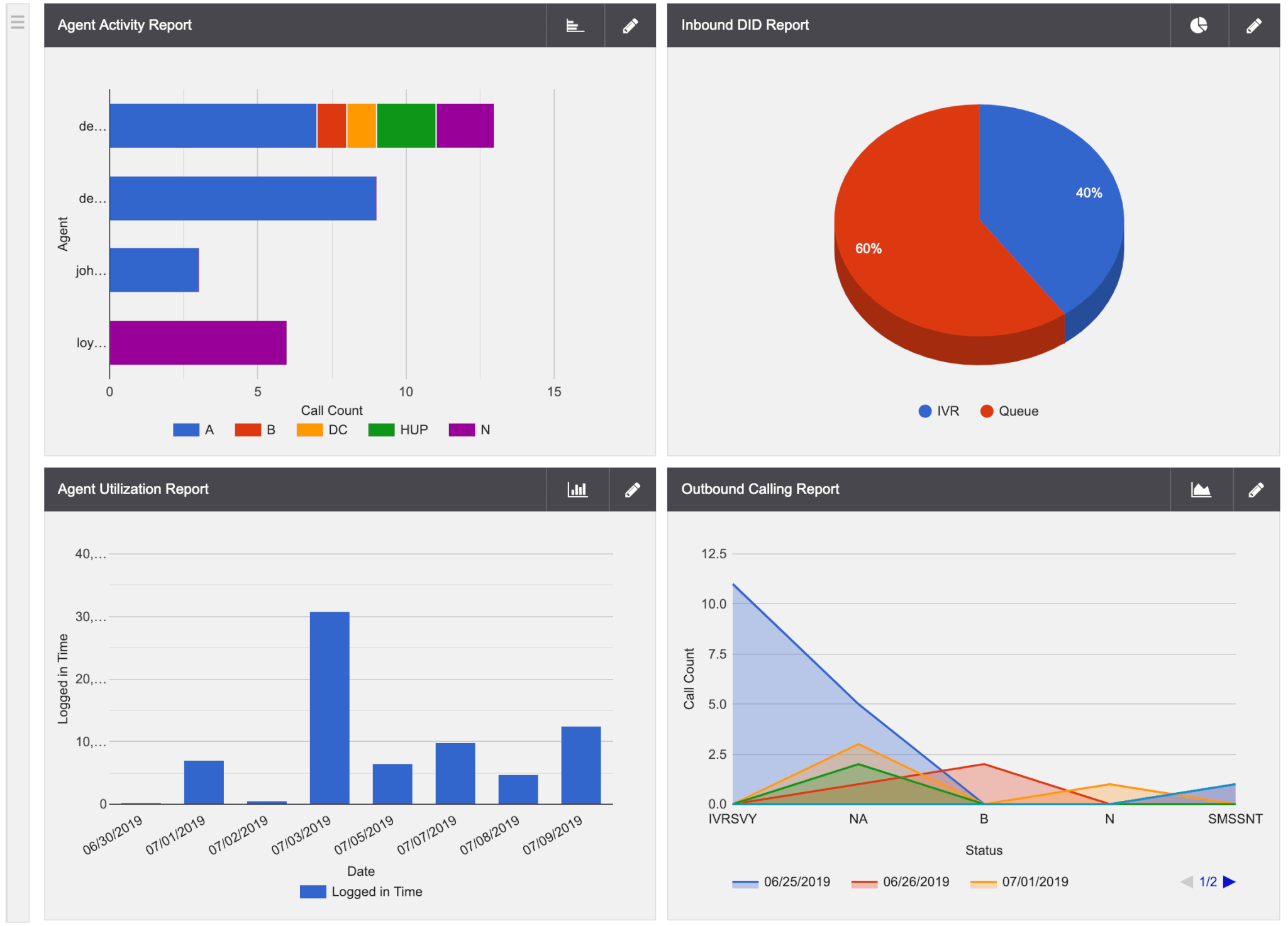
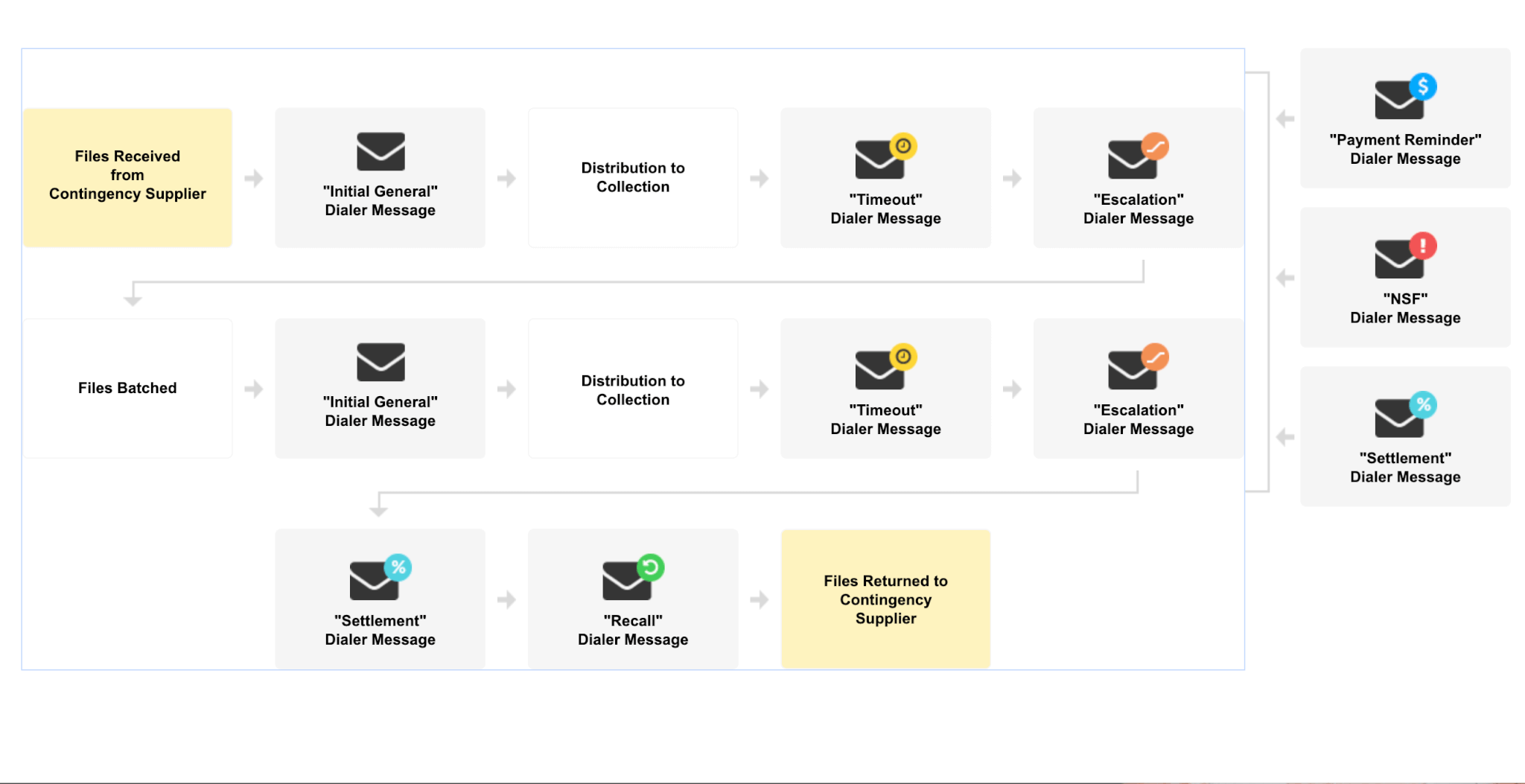
Monitor campaign and agent metrics in real-time to start making measurable improvements. Automate collections with built-in payment capabilities.
Powerful communication tools at your fingertips
Ready to build better conversation?
Learn about all the ways we can help you boost productivity, increase sales and start engaging with more customers.